Synthesis Repertory
Trusted worldwide by countless Homeopaths!
Quality • Precision • Flexibility • Reproducibility • Integration • Collaboration
Synthesis Repertory has been successfully used by Homeopaths worldwide since 1987. It is widely appreciated and respected thanks to its integrative and precise approach; uniting the work of the best contemporary homeopaths with classical sources, synthesised with meticulous attention to detail at every stage.
Synthesis Adonis has arrived with RadarOpus v3.0!
Synthesis Adonis is the successor of Synthesis Treasure Edition 2009V and is a major step forward, offering the fruits of over 12 years work of our team! A wealth of information has been added, many corrections have been executed and some innovative new ideas are included in this version.
Watch the video - Everything you always wanted to know about Synthesis – a dialogue with Dr. Frederik Schroyens, the creator and editor of Synthesis
At this page you can learn more about:
- The HIGHLIGHTS of Synthesis Adonis
- The HISTORY of Synthesis Repertory
- The emphasis on RELIABILITY and QUALITY
- Linking repertory additions to the SOURCE Materia Medica
- Limiting Synthesis to specific 'VIEWS'
- The extensive network of CROSS REFERENCES and SYNONYMS
- Making your own Repertory ADDITIONS
- Adding FAMILIES to Repertory Rubrics
- Who CONTRIBUTES to Synthesis?
- WHAT'S NEW in RadarOpus v3, or read our BLOG for a shorter read
TIP - use the back key on your browser to return to this menu at any time.
| Synthesis comparison | ||||
|---|---|---|---|---|
| Synthesis version | Synthesis Adonis (2022) |
Synthesis Treasure edition Vet (2009) |
Essential Synthesis (printed) |
Core Synthesis (2016) |
| Number of remedies described | 3.233 | 2.375 | 1.990 | 149 |
| Author references | 1.599 | 905 | 583 | 636 |
| Veterinary information | Printed separately | |||
| b-bg only rubrics | ||||
| Remedies copied to superrubrics | ||||
| Kent's Treasure | ||||
| Global size comparison | 125 % | 100 % | 75 % | 50 % |
Synthesis - the backbone of RadarOpus!
Essential facts about Synthesis
RADAR was created in the early 1980's
- Synthesis has been at the core of its development since the very beginning
- Synthesis contains repeatedly checked additions from the classical homeopathic literature, including Kent, Hahnemann, Hering, Allen, Clarke, Boericke, Knerr, etc.
- Additions from contemporary authors are added only with caution, most often only in the first degree unless confirmation of a higher degree comes from other authors
- Each new version has been the fruit of thousands of hours of work by many dedicated people
- Every version of Synthesis is used millions of times by leading homeopaths before it is used to build another edition.
- As can be expected from these critical minds, they have checked the rubrics and the remedies repeatedly. Their comments are integrated into each new edition
- Synthesis has been enlarged by additions, but only 15% to 30% at each step.
- It is this policy that is the key to the exceptional quality of our Repertory
- Synthesis is available in hard copy and digitally - exclusively in RadarOpus!
- Our latest version - Adonis - is not yet available in print!
Teachers, practitioners & students all over the world are using Synthesis Repertory for their daily Homeopathic work. Why?
Highly reliable
The focus in Synthesis is to strike a balance between the classical and modern for the utmost quality and reproducibility in Homeopathy.
Edited by Dr Frederik Schroyens, a renowned Homeopath and Medical Doctor. He is an experienced and busy Homeopathic Doctor alongside his role in creating and editing Synthesis.
I believe we should take a resolute stand and treat each other's "fever for additions". Moreover, we should balance it with "fastidiousness about correct additions" ... It is misleading to call any Repertory complete. More work will always be needed to further improve the quality and increase the content of Synthesis. It is certain that this job will never be completely finished. As a consequence, all current collaborators and, in fact, anyone is invited to go on with this collaboration. The most productive contributions are made when everyone does what interests him or her: the remedy he needs, the author she likes, etc.
Dr Frederik Schroyens

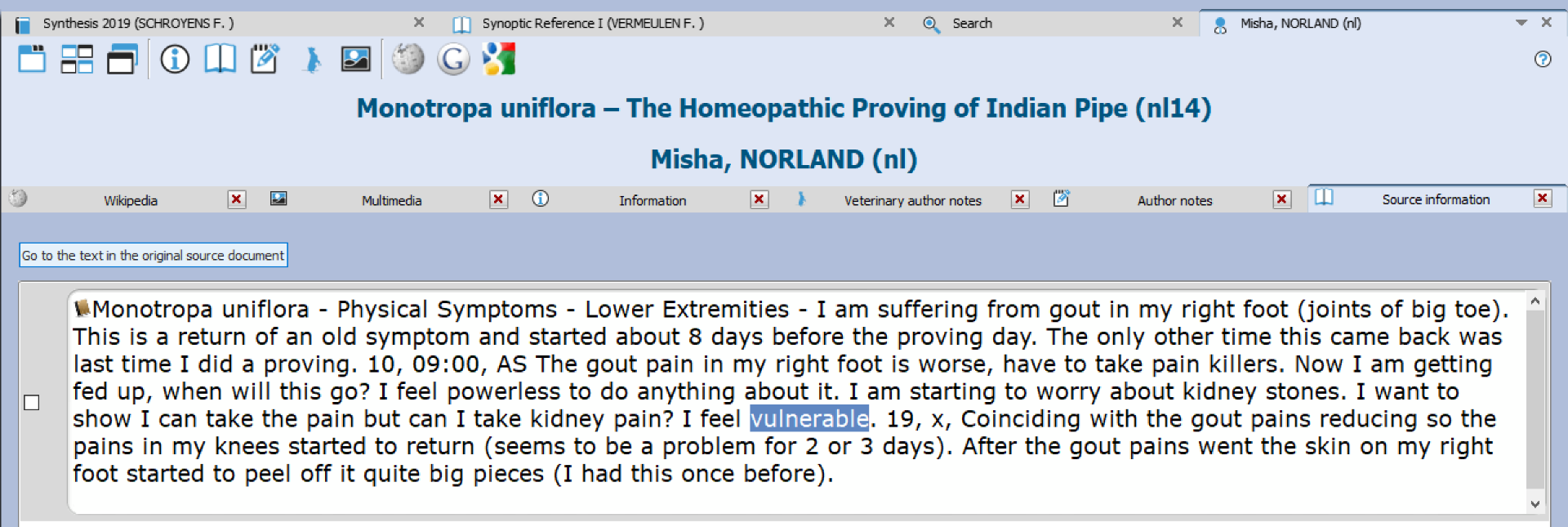
Every source is just one mouse click away
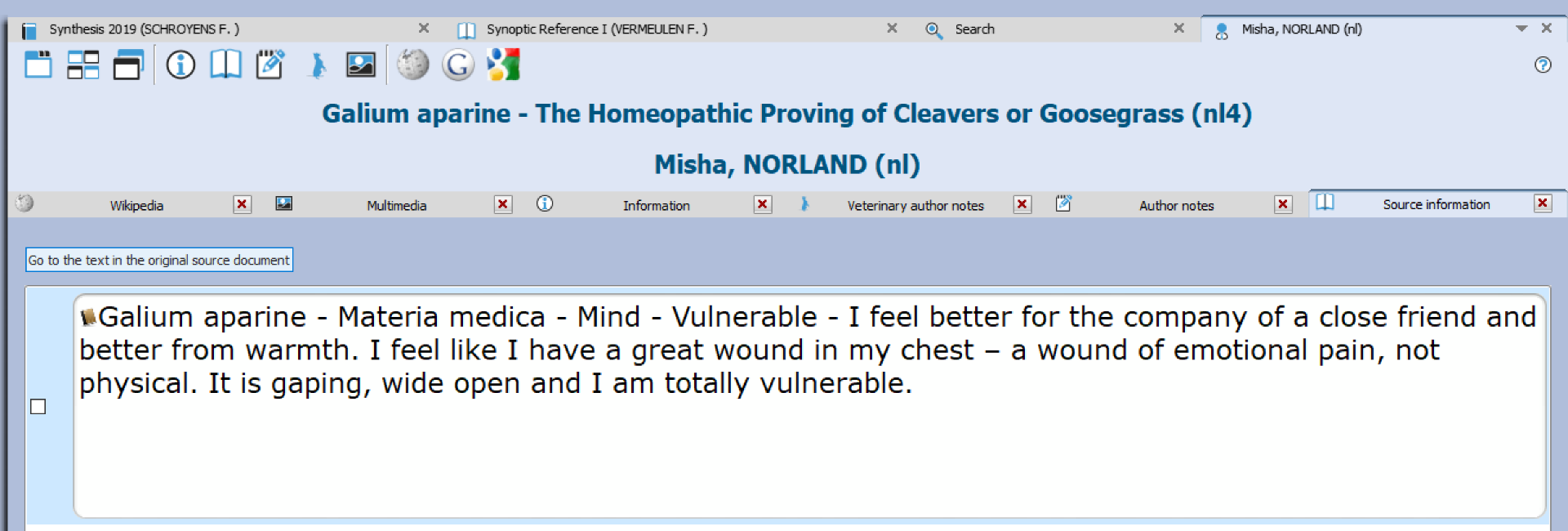
Synthesis is the only repertory allowing you to include explicit source information when making additions!
Not only precise bibliographical references, but also the actual text on which your Synthesis addition has been based. This is a most important tool to guarantee the quality of the additions by creating transparency and linking Synthesis and any Materia Medica in two directions. These additions can be shared between users, so that the Homeopathic community can collaborate on updating the repertory.
Integrated timeline - stick to the classical authors with a mouse click
Synthesis represents close collaboration throughout the profession
Experienced Homeopaths have contributed to the project by including their own valued clinical findings. The Synthesis team then draws together these reliable additions and combines them with high quality Provings that have been overseen by experienced Homeopaths. Within Synthesis, there is also the facility to limit the repertory to a “View”; which filters out additions of modern remedies for those who wish to stay rooted in classical provings.
Synthesis is based on Kent's Repertory and adds a vast amount of corrections and additions to it. We believe that it adds much more to homeopathy as a whole so that we can structure our homeopathic knowledge for the best, so it may be easily readable, transparent, and consistent.
We sincerely hope this instrument may help you in raising your homeopathic efficiency to a new level. After the knowledge of the Materia Medica, the use of the Repertory is the next best friend to allow the marvel of homeopathic cure to happen. We haven't spared any effort so that this Repertory may help homeopathy "grow brighter".
Dr Frederik Schroyens
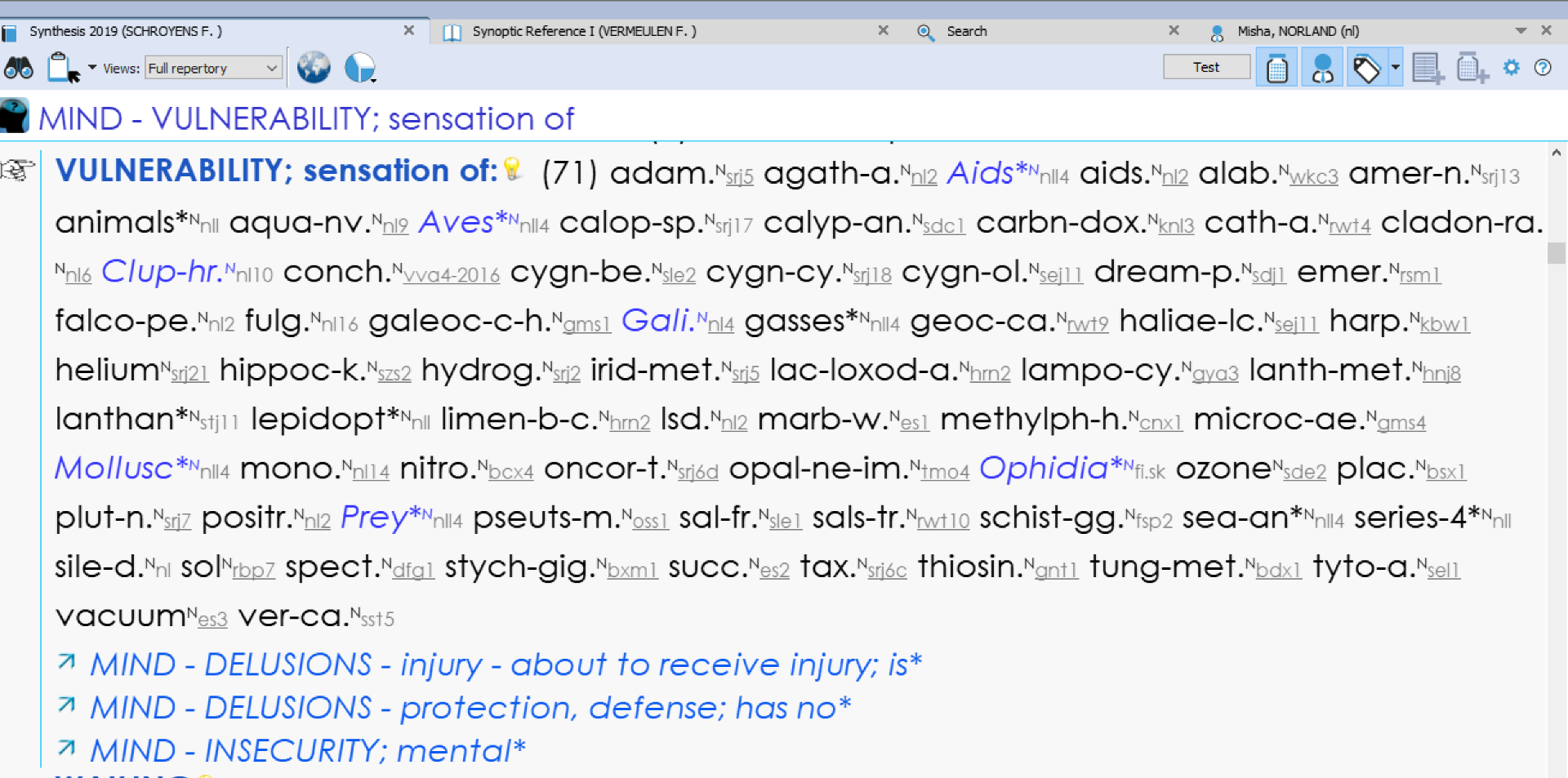
Jump to cross-references and synonyms
Race around the repertory with our extensive network of cross references!
Navigating Synthesis becomes easier even for newcomers, highlighting new rubrics for you to discover. Synthesis also includes many associated concept files which are designed to help you find rubrics. This is a great help for novices to the repertory who are yet to master the Victorian language employed! These concept files provide an alternative route into finding rubrics. You can search for a medical term or modern expression and find a link to the rubrics that cover the symptoms. Synthesis contains clinical and modern terms as these can be very helpful to modern Homeopaths.
Customise Synthesis with your own additions!
Quickly add remedies & new symptoms to Synthesis!
In Synthesis Adonis, you can also easily add your own:
- Cross-references
- Synonyms
- Personal Notes
- Additions to the Personal Chapter
- Add symptoms on the fly or even build your own repertory within Synthesis
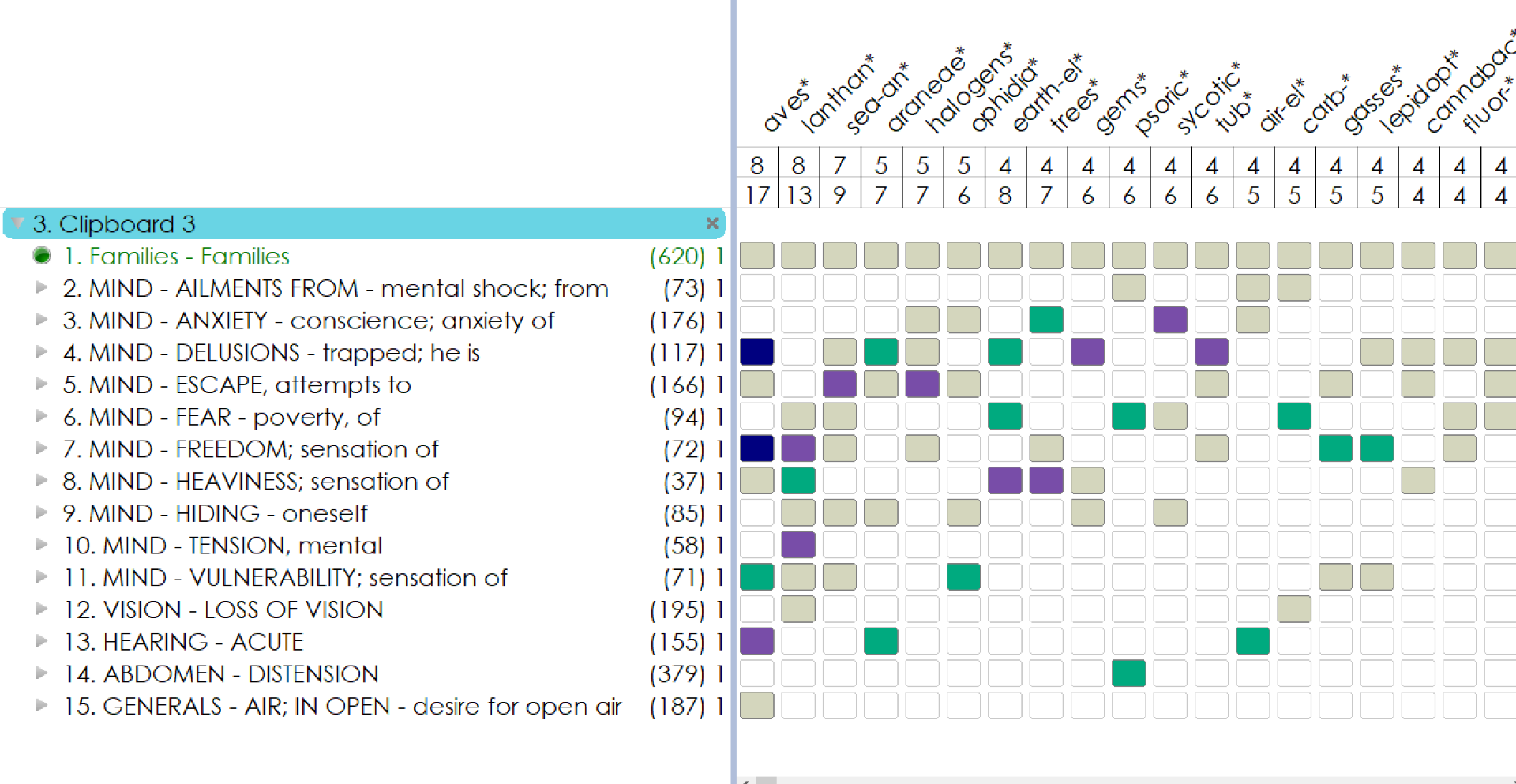
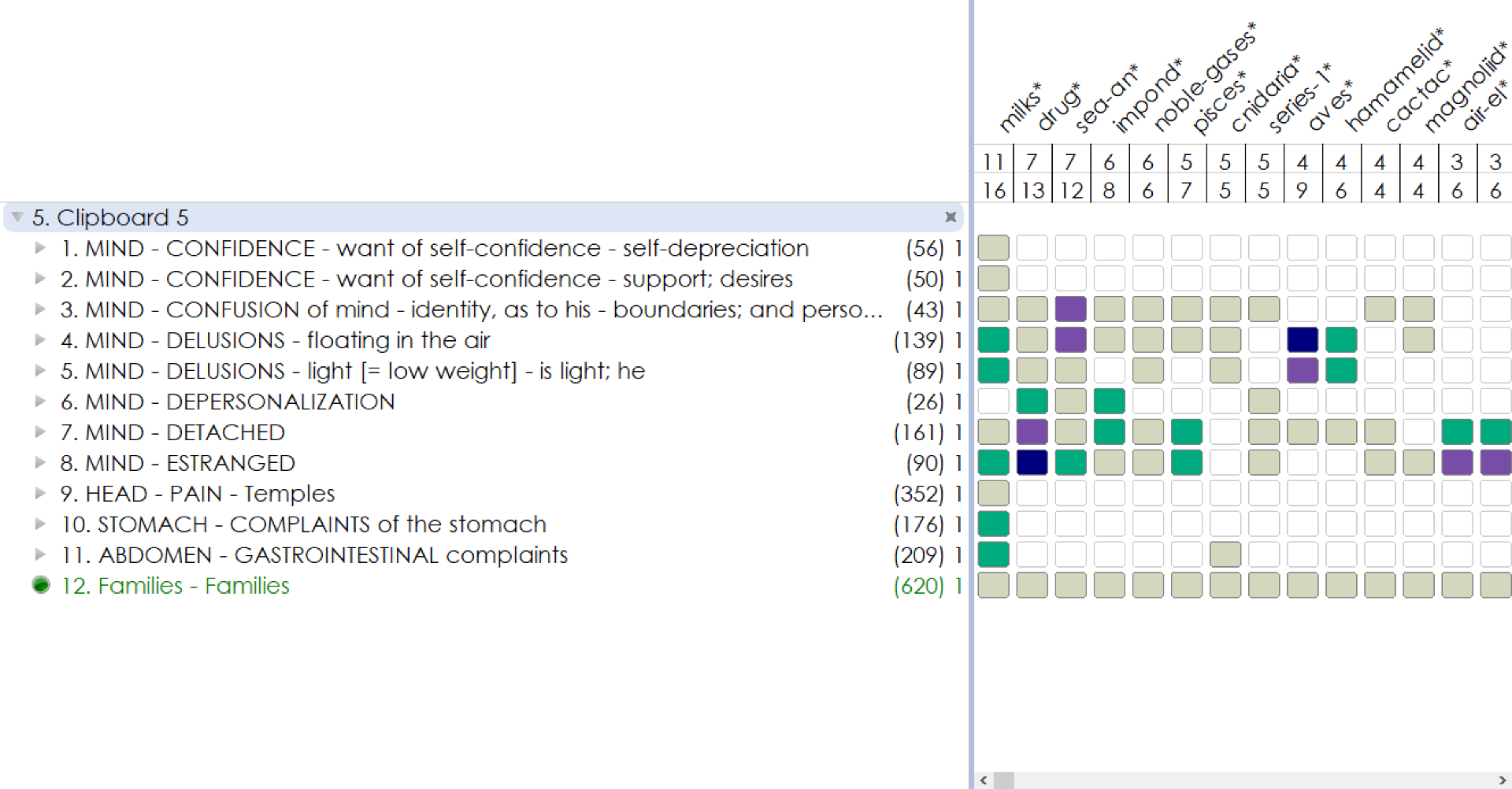
Add families to the repertory
Modern developments in Homeopathy have focused on groups or families of remedies and their shared characteristics
This has opened up many smaller remedies that may have been missed in the past. Lachesis has been prescribed countless times where perhaps other snake remedies may have been better suited, despite being under-represented in the repertory. Now you can add Families to rubrics based on your understanding of Kingdoms and families. The freedom to add any family to Synthesis makes it a truly unique repertory.

Collaborative approach
We like to work collaboratively with Homeopaths who share our vision for integration, quality and consistency
Some authors whose clinical additions feature in Synthesis are:
F. Master, A. Saine, R. Morrison, Dr Ramakrishnan, P. Schmidt, F. DeGroote, O. Julian.
Some modern provings that have been added are those by:
J. Sherr, M. Norland, N. Herrick, T. Rowe, L. Klein, R. Sankaran, P. Fraser, J. Shore, L. Schulz, A. Schadde, P. Tumminello, A. Gray, M. Thakar, Eberle & Ritzer, CCRH, J. Huenecke.
Synthesis is truly a worldwide project. It is designed in such a way as to incorporate the efforts of homeopaths of all countries and all languages, be it their personal additions, their work in the literature, or their comments and corrections. We centralize all this information and advance together in all languages simultaneously!
Dr Frederik Schroyens